
In early April 2026, a Finnish study published in Acta Paediatrica spread at remarkable speed. Within days, it was presented across many media outlets and social networks around the world as proof that medical transitions worsen the mental health of trans young people. The article, signed by Sami-Matti Ruuska and colleagues and coordinated by Riittakerttu Kaltiala, was read more than 100,000 times in one month, immediately becoming the second most-read article in the history of this journal, founded in 1921. The interpretation given by its media amplifiers was this: gender-affirming care deteriorates young people’s mental health. The problem is that nothing in the study could justify that conclusion, because their mental health was not measured, and the effects of their care were not estimated. Worse still: the transphobia these young people may face in everyday life – and sometimes within the healthcare system itself – was erased from view.
A Widely Read, Widely Quoted Study, But Much Less Solid Than Claimed
The impact was global. In France, for example, several media outlets almost immediately presented the study as proof that medical transitions for trans young people do not work, or even worsen their mental health. Breizh-Info spoke of an “explosion of psychiatric disorders”. Valeurs Actuelles presented the study as demonstrating “a deterioration in mental health”. Le Point spoke of “disastrous results” for young people’s health, claiming that “gender transitions generate or aggravate psychiatric pathologies”. In an interview, the same magazine folded the study into a broader critique of the recommendations of the Haute Autorité de santé. Atlantico and Village de la Justice used it within a framework in which medical transition is suspected of producing or worsening psychological suffering. Within weeks, a registry result had become a weapon in a public controversy.
The problem is that this media narrative rests on a major slippage: the study by Ruuska and colleagues does not directly measure young people’s mental health. It essentially measures the existence of contacts with specialist psychiatric services. That is profoundly misleading.
A psychiatric contact is not depression. A psychiatric contact is not a suicide attempt. A psychiatric contact is not a decrease in quality of life. A psychiatric contact is not necessarily a sign of deterioration. It may be an assessment, follow-up, coordination, helpful care, an access route, an administrative obligation, care for a pre-existing condition, or simply the effect of one group being observed much more closely than another.
The entire controversy turns on this distinction. The study was read as if it demonstrated that medical transitions worsen young people’s mental health. It does not. It observes that young people referred to specialist gender identity services in Finland more often had contacts with specialist psychiatry than cisgender controls, before and after their first contact with those services. That is an important finding. But it is not evidence of a harmful effect of treatment.
What the Study by Ruuska and Colleagues Actually Does
The Finnish study is based on national registries. Nordic registries make it possible to follow large populations over long periods, with fewer losses to follow-up than in many clinical studies. Ruuska and colleagues identify 2,083 people under the age of 23 (more than half of whom were legal adults) who contacted specialist gender identity services in Finland between 1996 and 2019, and compare them with matched cisgender controls.
Participants are divided into several categories, notably according to whether or not they received medical gender reassignment. The authors then examine whether these people had contact with specialist psychiatric services before the index date, and again at least two years after that date.
The index date is crucial. It is not the start of hormones. It is not the date of surgery. It is the first contact with a specialist gender identity service. In other words, the study does not compare mental health “before treatment” and “after treatment”. It compares psychiatric contacts before and after entry into a specialist pathway.
The authors could have proceeded differently. Finnish registries do in fact make it possible to identify dates of hormone dispensing through reimbursement databases. A strategy more directly suited to the question of treatment effects would have anchored the analysis to the actual initiation of gender-affirming hormone therapy, or to the date of a relevant medical intervention, and then compared trajectories before and after that exposure. They could also have distinguished more finely between periods of assessment, waiting, and actual treatment. Choosing the date of first contact with the clinic is not illegitimate if the goal is to study the overall pathway of young people referred to gender services; but it is not appropriate when one seeks to learn something about the specific effects of medical treatments.
This distinction is essential. In a long, psychiatric, and sometimes highly selective pathway, months or years may pass between first contact and actual access to treatment. A person can therefore ultimately be classified in the “treated” group while having accumulated psychiatric contacts after the index date but before any medical treatment. If these contacts are then interpreted as psychiatric needs “after medical transition”, the causal inference is considerably weakened.
The other decisive point is the measure itself. Ruuska and colleagues speak of “psychiatric morbidity” and “need for psychiatric treatment”. But the variable actually studied is the existence of at least one contact with psychiatric services, excluding appointments with the multidisciplinary gender identity team itself. This choice is far less solid than it appears. Even if appointments with the gender team are excluded, the psychiatric contacts that this specialist care generates downstream are not necessarily excluded: referral to a local psychiatrist, additional assessment, follow-up for a co-occurring disorder, stabilization consultation, and so on.
Here again, the authors could have used other indicators available in the registries, for instance the number of psychiatric contacts rather than a simple binary variable, recorded psychiatric diagnoses, psychiatric hospitalizations, emergency department visits for psychiatric reasons, or prescriptions of psychotropic medication. Such measures would have come closer to the severity, nature, or evolution of psychological difficulties than the simple fact of having had at least one contact with specialist psychiatry. But this was not done, or not shown.
The study by Ruuska and colleagues therefore does not make it possible to observe a worsening effect of gender-affirming care on young people’s psychiatric needs. More seriously, the effect it observes could stem from the systemic transphobia that trans young people experience once their transition pathway has begun, or even from the structural pathologization of gender-affirming care pathways in Finland.
Erin Reed’s Almost Immediate Fact-Check
On April 7, 2026, almost immediately after the study’s publication and viral spread, journalist Erin Reed published a detailed fact-check. Its title: “Fact Check: New Finnish ‘Study’ Does Not Prove ‘Trans Youth Care Leads To Worse Outcomes’.”
In her article, she shows that the study measures psychiatric appointments, not deterioration in mental health, since the chosen indicator does not directly inform us about the psychological state of the people followed. A one-off assessment, regular follow-up, or more intensive care are thus aggregated into the same category, reduced to a binary piece of information: was there at least one contact with specialist psychiatry?
Erin Reed also emphasizes surveillance bias. In the Finnish system, trans young people referred to gender identity services are not ordinary young people observed from a distance. They enter a system in which psychiatry is omnipresent. The specialist teams in Tampere and Helsinki have historically been embedded in adolescent psychiatry. Young people are assessed, followed, sorted, stabilized, and sometimes referred to other psychiatric services. Cisgender controls, by contrast, are not subject to such a level of observation.
In epidemiology, this problem is classic: the more one observes a group, the more problems one detects in it. If one group is followed every three to six months by clinicians actively looking for psychiatric symptoms, while another group is not exposed to that surveillance, the first group will appear sicker, partly because it is being watched more closely. This is surveillance bias.
Although her journalistic tone may be perceived as activist, Erin Reed’s many methodological criticisms – poorly defined measure, surveillance bias, misanchored temporality, binary variable, confusion between service use and morbidity – were later taken up, in academic form, in several letters published in Acta Paediatrica. In other words, this was not merely an isolated reaction: several of her objections were echoed within the scientific debate itself. Yet this critical context was largely ignored by the press. Rather than engaging with a well-supported fact-check and discussing the methodological limits it raised, many outlets preferred a simplified and pseudo-scientific reading, presenting as established what was in fact a contested interpretation of the data.
Two Studies Published at the Same Time, Cited Nowhere: Saxby and Vega
The contrast is striking. At almost the same time, two other studies appeared in February 2026, two months before Ruuska’s. They also concerned gender-affirming hormone therapy and the mental health of young people. They did not say the same thing as Ruuska. They were far less widely picked up.
The first is the study by Karinna Saxby and colleagues, published in a journal of the Lancet group. It uses Australian population-level administrative data from 2012 to 2024. The authors identify 20,358 people who initiated estradiol-based hormone therapy and 11,883 people who initiated testosterone-based hormone therapy. The study examines changes in mental health service use and psychotropic prescriptions before and after initiation of hormone therapy.
The methodological difference from Ruuska is major: Saxby and colleagues anchor the analysis to actual initiation of hormone therapy, rather than to entry into a clinic or pathway. They use a dynamic difference-in-differences model, with future initiators as the comparison group. They examine trajectories, not just a binary indicator.
The result is nuanced. Mental health service use increases around the start of hormone therapy, which may reflect assessment and support requirements, but then decreases substantially over time. In the overall cohort, five years after initiation, people on testosterone use fewer mental health services and fewer prescriptions on average. Trajectories under estradiol are more heterogeneous, with an initial increase in prescriptions followed by a decrease.
The authors also examine separately young people who started hormone therapy before age 18. In this subgroup, the trends move in the same direction: mental health service use increases around initiation and then gradually declines over the following years, with no signal of lasting deterioration associated with treatment. Most importantly, the authors explicitly write that service use does not directly capture underlying need. This is precisely the precaution that Ruuska and colleagues do not clearly formulate.
The second study, signed by Agus Vega and colleagues, was published in the International Journal of Transgender Health. It is based on a cross-sectional online survey in the United States of 5,178 trans women, transfeminine people, and non-binary people assigned male at birth. Participants are divided according to whether they initiated hormone therapy before age 18, at age 18 or later, never initiated it but desired it, or did not desire it.
Vega and colleagues do not conduct a strong causal study: the survey is cross-sectional, self-reported, and subject to selection bias. But its measures are more directly clinical and subjective: moderate-to-severe depression, appearance congruence, and comfort with how others perceive one’s gender. The results are telling: moderate-to-severe depression is higher among people who desire hormone therapy without having accessed it than among those who initiated it.
In adjusted analyses, people who began hormone therapy before age 18 also show more favorable indicators than those who desire it but have not accessed it: they less often report moderate-to-severe depression and have better scores for appearance congruence and comfort with others’ perception of their gender. Appearance congruence and comfort in others’ gaze are also lowest in the group that wants hormone therapy but has never accessed it.
This study does not prove that starting hormones in adolescence causes better long-term outcomes. But it shows a reality that the media narrative around Ruuska erases: non-access despite desire may be associated with the worst indicators of mental health and congruence. Delay or absence of care is therefore not automatically protective.
Ruuska was read more than 100,000 times in one month. Vega barely exceeded 200 views. Saxby and Vega went completely unnoticed in the press. The difference in attention does not necessarily reflect methodological quality. It reflects the political portability of the message. A study that can be summarized as “transition worsens mental health” travels much faster than a study saying, “service use increases around entry into care and then decreases over time”, or another saying, “people who want hormone therapy without accessing it are doing particularly badly”.
The Three Critiques Published in Acta Paediatrica
Nearly two months after Erin Reed’s fact-check, three critical letters were published in Acta Paediatrica: Edmiston and colleagues, Sandri and colleagues, and Banos and colleagues. They do not say exactly the same thing, but converge on one central point: the study by Ruuska and colleagues overinterprets an indicator of psychiatric service use.
In addition, Sandri and colleagues remind readers that the study does not measure the primary aims of gender-affirming care: reduction of dysphoria, improvement in bodily congruence, quality of life, and psychosocial functioning. Even if the study showed persistent psychiatric disorders, that would not be enough to conclude that care fails on its own objectives. Hormone therapy may reduce dysphoria without resolving depression linked to harassment, family rejection, poverty, violence, or trauma. This is a basic clinical nuance: a treatment does not have to cure every problem in a person’s life to be beneficial for the indication it targets.
The letter by Banos and colleagues is the broadest. It emphasizes not only methodological problems, but also ethical and editorial issues. Its starting point is that Ruuska’s title and framing may mislead: speaking of “psychiatric morbidity” while measuring psychiatric contact is problematic, especially in a politically explosive field.
Banos and colleagues underline that the Finnish gender identity system is structured by psychiatry. Assessments explicitly seek to identify, stabilize, or treat psychiatric disorders before authorizing certain treatments. Psychiatric contacts may therefore be produced by the pathway itself. In such a system, psychiatric contact is not only a property of the patient. It is also a property of the dispositif.
Their letter also raises selection bias and collider bias. Young people referred to gender services are not a random sample of trans young people; they are people who have entered a very specific system. The comparison with cisgender controls may therefore primarily measure the effect of being captured by a psychiatrically structured specialist pathway.
Banos and colleagues finally criticize the two-year threshold after the index date. In a long pathway, the two years following first contact may still correspond to assessment, waiting, a pre-treatment phase, or a real-life experience. Psychiatric contacts observed from that threshold cannot therefore simply be attributed to the effects of medical transition.
Worse still: if the pathway itself is long, uncertain, conditional, pathologizing, or experienced as hostile by some people, then it may contribute to the distress it later measures. This is the institutional iatrogenic hypothesis: suffering would not be produced by hormones or surgeries, but by the way access to care is organized, delayed, conditioned, or monitored.
The Response by Ruuska and Colleagues
In their response, Ruuska and colleagues argue that their critics partly misunderstand the Finnish healthcare system, registry-based research, and the scope of their study. They state that their study addresses methodological gaps by using a large national cohort, long follow-up, and appropriate comparison groups.
They then defend the use of contacts with specialist psychiatry as a measurement variable. According to them, in Finland, access to specialist psychiatric services is reserved for severe disorders, according to standardized national criteria; mild and moderate disorders are managed in primary care; and specialist follow-up ends after remission. They therefore conclude that the use of specialist psychiatric services constitutes a robust proxy for current severe psychiatric morbidity.
This is their central defense. It is also the most contestable point.
The fact that access to specialist psychiatry is regulated does not automatically turn psychiatric contact into a valid measure of morbidity. It does not tell us what the contact means in a population exposed to a pathologizing assessment pathway. Yet the authors had other information in the registries that they could have used differently. As several critics noted, the data made it possible to identify hormone prescriptions and therefore to anchor the analyses to the actual start of treatment rather than to first contact with the gender clinic. They could also have used the frequency or intensity of psychiatric contacts more finely instead of reducing them to a binary “at least one contact” variable.
These alternatives would not have removed all the limitations of registries, but they would have come closer to the question actually being debated: changes in mental health around the treatments themselves, rather than the mere fact of having been in contact with specialist psychiatry. The fact that Ruuska and colleagues – including in their response – provide no explanation for declining to use finer measures that were nevertheless available seriously weakens the credibility of the study and the general scope of the claims that can be derived from it.
Ruuska and colleagues also respond to surveillance bias by stating that referral to gender identity services does not require a specialist psychiatric assessment and can be initiated in primary care. They add that Finnish adolescents undergo mental health screening in schools, which would make it implausible that severe disorders would remain undetected except through the gender pathway.
This response does not solve the problem. Critics are not only saying that entry into the clinic requires specialist psychiatric assessment. They are saying that the pathway, once begun, produces surveillance, assessments, referrals, contacts, access conditions, and interactions with psychiatry. School screening does not generate the same level of follow-up as a specialist pathway centered on young people whose access to care partly depends on psychological stabilization.
Ruuska and colleagues acknowledge that minority stress may contribute to the results, but argue that the magnitude of the observed differences – several dozen percentage points – makes it unlikely that these factors fully explain them. They add that their study “does not claim definitive causality,” but calls for exploration of mechanisms, including possible adverse effects.
This caution is welcome, but it does not always match how the article was received, nor even certain passages of the article that are controversial. The conclusion that psychiatric needs “do not subside after gender reassignment” was considered problematic because it suggests a trajectory of psychiatric morbidity even though the study does not measure that morbidity. The repeated use of the term “psychiatric morbidity” in the title and abstract misleads readers who will not have read the full article. Exploring the possibility of adverse effects is legitimate. Presenting it in the media as if it had been demonstrated is not.
This response, however, leaves aside a central point: several of the results presented as especially concerning rest on crude comparisons between periods or groups, whose interpretation depends heavily on the composition of the cohorts. This is particularly true of the analysis around the year 2010.
The 2010 Turning Point: More Psychiatric Pathology Among Young People, or a Change in Population?
A significant part of Ruuska and colleagues’ argument rests on a temporal comparison: people referred to specialist gender identity services after 2010 had more contacts with specialist psychiatry even before their first contact with gender services, compared with people referred before 2010. In their response to critics, the authors explain that this cutoff corresponds to a documented increase in referrals to gender clinics in Western countries in the early 2010s.
The stakes of this date are considerable. In public debate, “after 2010” is not just a statistical period. It has become a political marker: the marker of the rapid increase in adolescent requests, of the relative feminization of referred cohorts, of the arrival of young people assigned female at birth, often pubertal or post-pubertal, and of the recurring fear of a “new” social phenomenon. If young people referred after 2010 appear more often in contact with specialist psychiatry before entering the gender clinic, some commentators see this as proof that the “new cohort” is intrinsically more fragile, that contemporary requests are more pathological, less “authentic”. That is why this temporal analysis must be examined with great caution.
The first problem is a possible composition effect. People referred before 2010 and after 2010 may not be the same populations. They may differ by age at first contact with specialist services, sex assigned at birth, pubertal stage, ability to formulate a request, or the social norms that make it more or less possible to come out as trans during adolescence. If, for example, recent cohorts include more young people assigned female at birth, referred during or after a bodily more rapidly visible puberty – breasts, periods, social sexualization – it is plausible that they would present more distress or psychiatric contacts even before entering the pathway. In that case, the increase observed after 2010 does not prove that “morbidity” increased in comparable populations: it may reflect the fact that the referred population changed.
Ruuska and colleagues’ response does not resolve this point. Saying, as the authors do, that the temporal cutoff corresponds to a real increase in referrals to specialist services in Western countries explains why 2010 is a relevant date, but it does not exclude a composition effect. On the contrary, the increase in referrals is precisely the context in which a change in composition becomes plausible: when a pathway scales up, the profiles entering it may also change. To neutralize this argument, it would have been necessary to show that the difference in pre-index psychiatric contacts before and after 2010 persists after the various adjustments. This specific analysis could have been conducted, but was not presented.
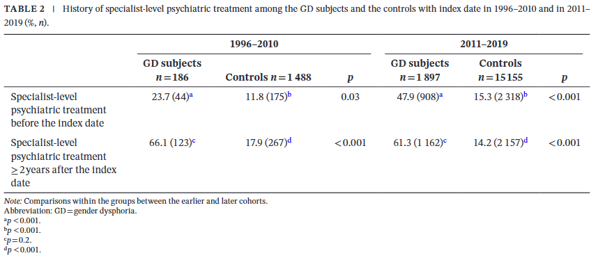
The second problem concerns the statistical reading of Table 2. The table gives the impression of a sharp increase in “psychiatric needs” in recent cohorts, but some useful comparisons are not tested. In particular, the post-index proportion in the group referred before 2010 is 66.1%, compared with 61.3% in the group referred after 2010. This difference even goes in the opposite direction to a post-2010 worsening and, when tested approximately as a difference in independent proportions, is not statistically significant. In other words, the striking contrast in the table is not that psychiatric contacts exploded after 2010; it is mainly that the pre-index level was much lower (23.7%) in the older cohort and much higher (47.9%) in the recent cohort.
One can also compare the apparent “worsenings”: 66.1% – 23.7% = +42.4 points before 2010, versus 61.3% – 47.9% = +13.4 points after 2010. The crude worsening appears much larger in the older cohort. But this calculation cannot be properly tested from the published margins alone, because the data are paired: the same people are observed before and after the index date, and the table does not say who moves from “no contact” to “contact”, who remains in contact, who exits care, or who enters care. A naive approximation assuming independence yields a statistically marked difference, but it is driven mainly by the low baseline of the older cohort. To interpret these trajectories properly, one would need the individual-level data or at least transition tables. Once again, this analysis could have been conducted, but no result is shown.
If one reads the table superficially, one can tell a simple story: after 2010, referred young people were more psychiatrically fragile, and this fragility remained high despite, or even because of, care. But another reading, just as compatible with the figures, is that the old cohort and the new one are not comparable: the first starts from a very low baseline and reaches a post-index level close to the second; the second already enters the system with more prior psychiatric contacts. This may simply reflect a change in the profile of referred people.
This point is decisive for public debate. Another explanation, compatible with the available data and much less pathologizing, is that the turn of the 2010s mainly changed the composition of cohorts referred to specialist services. The improvement in transgender visibility from the 2010s onward may have produced two simultaneous effects. On the one hand, it may have helped depathologize some forms of childhood gender non-conformity, historically more often noticed and referred when they concerned prepubertal children assigned male at birth: a boy perceived as “effeminate” more easily worried parents, schools, or clinicians than a girl perceived as a “tomboy”. On the other hand, the same visibility may have made adolescent requests for medical gender transition more speakable and accessible, especially when puberty makes dysphoria more concrete, more visible, and harder to avoid.
The data from Kahn and colleagues are consistent with this hypothesis: referrals to specialist services are more often AMAB in childhood, more often AFAB in adolescence, and then again more often AMAB in adulthood. In other words, the sex ratio of pediatric clinics does not necessarily reflect a sudden change in the trans population itself; it may reflect the age at which different people become visible, are noticed, come out, or can ask for help. In this context, comparing pre-2010 and post-2010 cohorts as if they were directly comparable is fragile: the former may have included proportionally more prepubertal children referred for gender non-conformity, especially AMAB, whereas the latter may have included more pubertal adolescents, more AFAB youth, and more young people explicitly formulating a request for medical transition linked to gender dysphoria. Such a transformation is enough to make an increase in psychiatric contacts at baseline plausible, without needing to assume a “social contagion” specific to trans youth in the 2010s. Ruuska and colleagues could have adjusted their model to account for age at index and sex assigned at birth, which would have made it possible to test this hypothesis, but this was not shown.
This mechanism must be formulated carefully. The point is not to say that AFAB young people are “by nature” more psychologically fragile than AMAB young people. A more robust formulation is that AFAB young people may be more likely to formulate, share, and have recognized a request for care during adolescence, because some pubertal changes – breasts, periods, hips, social sexualization – are early, visible, and sometimes experienced as difficult to conceal, whereas AMAB young people may be more prevented from coming out as transfeminine adolescents by transmisogyny and the social cost of transgressing masculinity.
This is precisely what the European data by Vandendriessche and Cohen suggest: at comparable age of LGBT self-awareness, AMAB young people come out as LGBT later than AFAB young people, and this gap varies according to macrosocial contexts and LGBT rights. Thus, a post-2010 cohort that is more adolescent and more AFAB may arrive in services with more prior psychiatric contacts, not because young people have become more “pathological”, but because social visibility has changed who enters clinics, at what age, with what request, and with what exposures already accumulated: pubertal dysphoria, school bullying, family conflict, access delays, stigma, or minority stress.
The analysis around 2010 shows a descriptive break in psychiatric contacts recorded before entry into gender services, but it does not allow one to conclude that young people in recent cohorts were intrinsically more psychiatrically “morbid” at comparable characteristics. To support such a conclusion, a specific reanalysis of baseline by cohort would be needed, adjusted for demographic and clinical composition, as well as a longitudinal analysis of individual transitions in psychiatric service use. These analyses were possible, but were not shown.
Alternative Causal Hypotheses
Regarding the main result of the study by Ruuska and colleagues, the problem is not only that the authors do not prove a negative effect of treatments. It is that several alternative causal stories are compatible with their results.
1. Minority Stress
Trans young people are exposed to higher levels of harassment, family rejection, violence, institutional discrimination, anticipated rejection, and barriers to care. These factors can produce depression, anxiety, self-harm, suicidality, and psychiatric service use.
For Vega and colleagues, the mental health burden of trans people is rooted in individual but also societal and structural factors, including stigma, abuse, family exclusion, institutional transphobia, and barriers to care. This perspective makes it implausible that a medical treatment alone should make all psychiatric morbidity disappear.
The minority stress explanation is compatible with Ruuska’s results. It explains why young people referred to gender services already have more psychiatric contacts before the index date. It also explains why these contacts may persist, or even increase, after the index date. Indeed, this date likely corresponds to the beginning of a gender transition pathway, whether medicalized or not, and often to a period when gender identity becomes more socially visible. Coming out, changing one’s name, changing gender presentation, or starting transition-related steps can expose a person to more transphobia, rejection, discrimination, and violence than when identity remains hidden.
In the Finnish context studied, people were also subjected to a period of real-life experience, that is, an experience of living in the affirmed gender before certain treatments. Such a requirement may increase exposure to hostile reactions from one’s surroundings, to school or workplace difficulties, and to minority stress. From this perspective, an increase in psychiatric contacts after the index date could reflect not a harmful effect of the treatments themselves, but the psychological consequences of increased visibility in a sometimes hostile social environment.
This argument is all the more reasoned because the increase in psychiatric contacts is not observed only among people who accessed medical transition (GR+). People in the GR- group, who were referred to gender services but did not receive medical gender reassignment according to the study definition, also show high levels of psychiatric contacts after the index date. This result is reinforced in the later analysis published in the response by Ruuska and colleagues, conducted only on follow-ups of five years or more.
This finding considerably weakens the hypothesis that medical treatments are the main driver of the observed results. If psychiatric contacts also increase among untreated people, this suggests that factors common to both groups – exposure to minority stress, increased visibility, discrimination, social rejection, family difficulties, or effects of the institutional pathway itself – play an important role. In other words, the data are entirely compatible with the idea that psychiatric contacts are largely determined by social and structural factors affecting trans people, rather than by the specific effects of medical interventions.
2. Gatekeeping Can Produce Suffering
A second story is more critical of the Finnish system itself. If access to care is long, uncertain, pathologizing, conditioned on the stabilization of symptoms, and experienced as a permanent inquiry into the legitimacy of one’s identity, then the pathway may produce distress. This distress may then appear in registries as “psychiatric contact”.
Erin Reed illustrates this hypothesis through several testimonies and accounts of Finnish young people’s pathways reported in her analysis. She notably describes young people reporting years of waiting, repeated assessments centered on their psychological difficulties, or the perceived need to demonstrate sufficient stability in order to hope to access treatment.
Some accounts describe worsening anxiety linked to the uncertainty of the pathway itself: fear of being refused, a feeling of being constantly assessed, the impression that every psychological difficulty may become an additional obstacle to accessing care. Reed also reports situations in which young people were allegedly referred to prolonged psychiatric follow-up before any decision concerning gender-affirming treatments.
These anecdotes recall an essential methodological point: when a care system itself generates psychiatric assessments, referrals, and follow-ups, the contacts recorded in registries may partly be the product of the institutional functioning of the pathway. In this iatrogenic hypothesis, it is not medical transition that worsens mental health; rather, the system of gatekeeping – the way care is conditioned, delayed, or monitored – is responsible. This means that a highly psychiatric system can create its own signals of morbidity.
3. Entry Into Care Increases Contacts
When a person enters a care pathway, they may have more medical or psychiatric contacts because their needs are finally identified. This is not necessarily deterioration. It may be the effect of better access.
Saxby shows precisely this kind of dynamic: mental health service use increases around the initiation of hormone therapy, then decreases over time. In this reading, the initial increase is compatible with assessments, support, and the identification of unmet needs. The long-term trajectory is more informative than the mere fact of having had at least one contact.
Ruuska and colleagues partly object to this hypothesis by presenting, in their response, a post hoc analysis five years after the index date. According to them, the persistence of an increased risk of specialist psychiatric contacts several years after entering the pathway makes it less plausible that the results are solely due to a transient phase of assessment or surveillance immediately after first contact with gender services. This argument weakens a narrow version of the hypothesis that the entire observed increase is nothing more than a short-term artifact linked to entry into the healthcare system.
However, it does not fully rule it out. First, the analysis remains anchored to the date of first contact with specialist services and not to the actual start of medical treatments. Second, an excess of psychiatric contacts at five years can still reflect several competing mechanisms: persistence of pre-existing vulnerabilities, lasting effects of minority stress, clinical selection of people referred to services, appropriate continuity of care for chronic disorders, or consequences of long and highly psychiatric pathways. Prolonged follow-up therefore reduces the explanation based on a mere initial assessment phase, but it does not allow the observed differences to be attributed to a specific harmful effect of medical transition.
4. Clinical Selection
Young people who obtain medical transition are not randomly selected. They are selected by a clinical system. Active psychiatric morbidity may delay or prevent access to treatment. This means that the GR+ group may have lower psychiatric use before the index date, not because it is intrinsically less vulnerable, but because the system selects people perceived as more stable or more able to move forward.
If this group then enters enhanced follow-up, it may accumulate post-index psychiatric contacts. The observed “gain” is therefore not evidence that treatment worsens mental health; it may be an artifact of selection and surveillance. In this hypothesis, the increase in psychiatric contacts mainly reflects a change in the intensity of detection and follow-up, rather than a real deterioration in psychological state caused by the treatment itself.
Medical Prudence Requires Rejecting Caricatures
It is possible to defend cautious medicine without falsifying what studies say. It is possible to recognize the psychological vulnerabilities of trans young people without concluding that their identity is a symptom. It is possible to ask for better data without turning a psychiatric contact into evidence of therapeutic failure. It is possible to discuss indications, delays, comorbidities, regrets, uncertainties, side effects, and care pathways without producing a moral panic.
The study by Ruuska and colleagues is worthwhile, but it does not deserve to be brandished as proof that medical transitions worsen young people’s mental health. The best reading is much simpler and much more demanding: in a healthcare system where trans young people are already highly selected, closely monitored, and heavily psychiatrized, many contacts with psychiatry are observed. To know what those contacts mean, we need studies that measure symptoms, dysphoria, quality of life, congruence, delays, refusals, violence, family support, treatment effects, and the effects of the system itself.
Saxby and Vega remind us that another scenario is possible: access to care may be accompanied by an initial increase in contacts because it opens doors, followed by a long-term decrease; people who desire hormone therapy without accessing it may be those doing worst; indicators of congruence and depression do not tell the same story as a simple psychiatric contact.
In an honest public debate, the Finnish study would be one piece among others. It would invite us to better understand the psychiatric pathways of trans young people, to improve support, to avoid iatrogenic delays, to measure valid constructs, and not to promise that transition will solve every problem in a life marked by stigma. It would not be used to claim that medical transitions worsen young people’s mental health.
Note: TYT science news articles are now written and translated with the assistance of artificial intelligence tools. Their content nevertheless rests on a systematic and complete human reading of the studies presented, ensuring the accuracy of the information and allowing the TYT team to contextualize, editorialize, and freely put current research into perspective.
More news
It Is False to Say That Medical Transitions Worsen Young People’s Mental Health
On the pseudoscientific exploitation of a study
Read more
Webinar “A Trans-Skeptical Parenthood” on July 2 at 6:30 p.m.
Trans Youth Trajectories webinar
Read more
2.2% of young people in France are trans or non-binary
Findings from a nationally representative survey
Read more
Photo display of trans and non-binary youth ‘Nous en image’ in Paris starting this Saturday
At the LGBTI+ center La Bulle
Read moreOpen letter to the American Society of Plastic Surgeons and to national and international professional health societies
About pediatric gender-affirming surgeries
Read more
More than a medical debate: How trans youth experience care and belonging
Inside a year of trans adolescence
Read more